English and Spanish Medical Languages:
A Comparative Study from a Translation Point of View
Lucía Ruiz Rosendo
Universidad Pablo de Olavide, Sevilla
Medicine is one of the most translated fields in Spain which is the logical consequence of importing scientific literature from Anglo-Saxon countries. For this reason, medicine constitutes in the new century an interesting field for translators, particularly for those whose language combination is English-Spanish. As a matter of fact, nowadays English is doubtless the language par excellence of medical science. In this situation, the translator is urged to master the specific features of medical language, both in English and in Spanish, in order to develop a high quality translation. Consequently we have carried out a deep analysis of the existent literature on medical language and thorough research in medical texts to provide a comparative analysis of English and Spanish considering the influence of English on Spanish medical language.
key words: medical language, translation, influence of English medical language, comparative study.
La medicina constituye uno de los campos más traducidos en España, consecuencia lógica de la importación de la literatura científica de países anglosajones. De este modo, la medicina representa en el nuevo siglo un ámbito de interés creciente para los traductores, especialmente aquellos cuya combinación lingüística es inglés-español. De hecho, actualmente el inglés es, sin lugar a dudas, la lingua franca de la ciencia médica. Ante esta situación, el traductor se ve obligado a conocer las características específicas del lenguaje médico, tanto inglés como español, con el objeto de desarrollar una traducción de calidad. Por consiguiente hemos llevado a cabo un análisis detallado de la literatura existente sobre lenguaje médico y una investigación exhaustiva en textos médicos para proporcionar un análisis contrastivo del inglés y del español teniendo en cuenta la influencia del inglés en el lenguaje médico español.
palabras clave: lenguaje médico, traducción, influencia del lenguaje médico inglés, estudio contrastivo.
I had never thought that the language used in [international scientific] exchanges would be a possible matter for debate. Certainly, it is a subject for historical analysis […]. But, languages? There is no plural in contemporary, top level, basic science: English is THE language of communication and it never occurred to me that anybody who knows anything about the dynamics of science today would even question the issue.
(Alberch 1996)
1. definition of specialised languages
Medical language is considered a specialised language or a language for specific purposes. According to Jiménez (2002), there is a spectrum of definitions of what a specialised language is in contrast to general language. This author offers a series of denominations both in Spanish and in English and highlights the influence of English even on the definitions. Some of the Spanish terms would be lenguas de especialidad (Cabré 1993), lenguajes especializados (Cabré 2002; Jiménez 2002), lenguas especializadas (Lerat 1997), lenguas especiales (from the English term special languages) (Rodríguez Díez 1979, Felber and Picht 1984), tecnolectos (technolects) (Arntz and Picht 1995; Congost Maestre 1994), lenguas profesionales (professional languages) (Felber and Picht 1984) or lenguajes científico-técnicos (language for science and technology) (Rodríguez-Díez 1979), lenguajes para propósitos específicos (language for specific purposes, LSP) (Cabré 1993) and lenguajes con fines especiales (language for special purposes) (Hoffman 1982; Sager 1993).
In order to be consistent throughout this paper, we will use from now on the acronym of the term language for specific purposes, LSP (Hoffman 1979). LSPs are usually studied in contrast to the general language. However, there is a lack of definition, but a broad range of comments is available, some of which we will analyse for they appear to be relevant to the particular subject of medical languages.
Hoffman (1979), one of the first authors who provided a definition, divides general language from specific and considers that LSP consists of a series of linguistic phenomena that take place within a given communication sphere limited by subjects, intentions and specific conditions. Nevertheless, Hoffman’s definition is not shared by other authors who consider that, just as specialised knowledge cannot be studied apart from general knowledge, LSP cannot be separated from general language. Thus, Cabré (1993) thinks that Hoffman’s position does not explain certain questions such as how frontiers between general language and LSP are established, which is the underlying concept of the term «general language» and whether the linguistic phenomena that differentiate LSPs from general language are convincing enough to maintain this separation.
According to Cabré, LSP refers to the ensemble of sub-codes, partially coinciding with the sub-code of general language, characterised according to some special peculiarities, that is to say, proper and specific features, like the topic, type of interlocutor, communicative situation, speaker’s intention, etc. An LSP would be, from a pragmatic point of view, a series of possibilities determined by the elements that intervene in each communicative act: interlocutors, communicative circumstances and intentions or purposes of the communicative act.
Picht and Draskau defend this position and define LSP as follows:
(…) a formalized and codified variety of language, used for special purposes and in a legitimate context –that is to say, with the function of communicating information of a specialized nature at any level -the highest level of complexity, between initiated experts, and, at lower levels of complexity, with the aim of informing or initiating other interested parties in the most economic, precise and unambiguous terms possible.
(Picht and Draskau 1985)
In short, we adhere to Cabré’s (1993) definition considering it a multidimensional and comprehensive definition that accounts for not only the differences and similarities of the general and specialised language, but also several aspects such as topic, communicative situation, speaker’s intentions and the means in which the communication act takes place.
2. the importance of english as ‘lingua franca’ of the international medical community
There is a broadly shared consensus on the predominant role of English in the international medical community (Sliosberg 1971; Fischbach 1986, 1993; López and Terrada 1990; Rouleau 1993; Aleixander et al. 1995; Navarro and Barnes 1996; Gutiérrez Rodilla 1997; Pilegaard 1997; Navarro 1997; Van Hoof 1999; Munday 2002; Snell-Hornby 2006). Without a doubt, over the last decades English has become the language par excellence of the medical science, displacing other languages, such as French or German. Nowadays, English is the language for communication in the field of health sciences, and has become a second common language for doctors and researchers and, in general, for all those people involved in scientific disciplines (Navarro 1997). For this reason, current scientific monolingualism constitutes a recognised and accepted phenomenon in the scientific community and in society.
In the 70’s, Sliosberg had already detected the increasing tendency for English to be used in medical language:
Les échanges internationaux font traverser aux mots les frontières et les océans et les font implanter dans les langues étrangères et l’extraordinaire essor scientifique et technique des Anglo-Saxons explique la pénétration des termes d’Outre-Manche et d’Outre-Atlantique dans les langues du vieux continent.
(Sliosberg 1971)
The influence of English in medicine can be possibly attributed to the predominant role of the United States as a neuralgic core of scientific and technological research where many new medical notions are created. Likewise this country controls the media in which the results from research are disseminated, namely the most important specialised journals and databases. Thus scientists from all over the world have come to accept the necessity of publishing their articles in English in order to be recognised and well-known.
(Gutiérrez Rodilla 1996)
Linguists interested in this phenomenon have proposed several names: lingua franca, second language, auxiliary language, universal language. English has even become not only the international language, but also an intra-national language of medical communication. In fact, scientists must not only write their papers in English in order to be published in international journals, especially American ones, but in the same country doctors who participate in conferences or write articles for national journals use English as a vehicle for communication.
In order to illustrate the predominant role of English in the current international medical scene, we have included the bar chart from Navarro (2002) which shows the rates of English bibliographical references in the journal Actas Dermo-Sifiliográficas for the period 1910-2000. This graph shows the increasing predominance of English in medical articles:
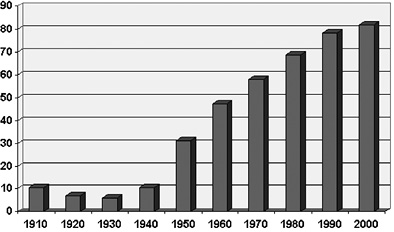
According to Navarro, this predominance involves a series of hidden consequences:
— The exclusion of papers written in other languages.
— The scientific dependence and the standardisation of thought, given that research lines, concepts, ideas and reasoning are determined by those international journals which are published in English and in whose editorial committees English native speakers by far out-number any others (75%). Consequently authors tend to choose their research topics, concepts and methodologies according to those followed in the United States, which leads to intellectual monolitism.
— The most important scientists publish the results of their research in English, which has favoured the creation of a linguistic barrier between high quality medical science, which is published in English, and that which is perceived as secondary, published in the mother tongue of the researchers. As a result, people tend to believe that an article written in English is better than an article written in another language.
— The excuse of poor style has been used to strengthen the world-wide supremacy of English native scientists.
— In Spain, texts are often written by authors who read in English and then have to translate key terms into Spanish, which jeopardises the quality of their papers. Scientists that read in English and publish in their mother tongue are not always aware of translating, or participating actively in the creation of neologisms and technical terms, and they write in an individual and disorganised way.
This hegemony of English can be found not only in the specific field of medicine. Thus certain authors have also highlighted the consolidation of English as the major global language of general, and not only medical, communication (Munday 2002). Munday attributes this status to the Internet, a communication means which is changing the role and visibility of translators and translations even offering nowadays (sometimes rudimentary) automatic machine translations of individual pages and of whole websites most often with English as the source language or target language.
By the same token, Snell-Hornby (2006) also underlines the influence of new technologies on the rise of English as language par excellence of general communication stating that «to the spread of English as lingua franca contributed the rapid developments in information technology that took place during the 1990s and the electronic world of the outgoing 20th century: multimedia, Internet, power-books and swatch-talk». This is what Benjamin Barber (1992) calls the McWorld as applied to language and communication, a sort of language which is to a great extent a particular brand of American English, reduced in stylistic range and subject matter, and - with the aid of abbreviations, icons, acronyms and graphic design- it is tailor-made for fast consumption. As aforementioned, the lingua franca in medical language is also American English. Perhaps this is due to a great extent to the worldwide domination of North American technology and culture and to the simplicity of its basic grammar and core vocabulary which can be relatively easily acquired for everyday conversation (Snell-Hornby 2006).
All in all, English has replaced other languages, such as Latin and French, as lingua franca not only of scientific community but also of general communication. The problem is that this standard English used worldwide by speakers from a wide range of countries usually is a hybrid language between the main English grammatical features and vocabulary and the characteristics, sometimes extremely different, of the speaker’s own mother tongue. Society is thus creating a brand new means of communication. A standard English that is not used in countries where English is actually the native language and which in some cases borders on artificiality and stylistic poverty. According to Snell-Hornby (2006) the use of English in everyday conversation as needed for superficial communication by speakers of other languages is «coupled with a structural flexibility in the language itself and a general policy of non-puristic openness among the English-speaking cultural institutions».
3. English and Spanish medical languages: differences and similarities
Along the lines of Navarro (2002) Spanish medical language does not escape the predominance of English, and nowadays it is impossible to analyse it separately from English medical language. In fact, given the situation described in the previous section, Spanish scientists have been urged to use English as their work language, for writing their own articles or for understanding other papers. For this reason, English has penetrated Spanish medical language in the shape of borrowings, calques, neologisms, etc.
This predominance is acknowledged by most authors. In this way, Gancedo (1994) affirms that, even if most of the terms coined in English could be translated into Spanish, without doubt the science is written in English and this language has dominated other languages, thus it is not reasonable to raise an objection to a consummated fact that has to be accepted as a practical measure that facilitates international communication and scientific progress.
We will now analyse the influence of English on medical Spanish language through a comparative analysis of their most relevant linguistic characteristics.
3.1. General features
Before analysing medical language features, we will examine the distinctive features of scientific language. This can be distinguished from other languages by virtue of some specific grammatical, lexical, semantic and stylistic demands: universal nature, accuracy, objectivity, lack of expressiveness and emotion, clearly defined meaning and connotation in order to avoid any kind of confusion and allow universal communication, lexical monosemic, appropriateness and correction, and clarity and precision. At the same time scientific language should use short sentences, avoiding excessive ideas in one same sentence, using well-known terms, and avoiding linguistic resources and literary figures. Likewise, it should be elegant and natural, with frequent repetitions given the fact that the main target is accuracy and clarity.
Medical language, as a scientific language, should respect these requirements, so it should be characterised by its accuracy and rigour and employ exact terms to avoid any kind of confusion and achieve universal communication. However, in the last few decades medical language has developed a series of linguistic phenomena that corrupt the language and bring about a loss of precision and clarity in the message, which constitutes one of the most important obstacles to medical training and research.
3.2. Lexical and semantic level
Polysemy and synonymy
The first striking similarity between English and Spanish medical language is the existence of polysemy, synonymy and homonymy for it contradicts one of the most important features of specialised languages: univocity of meaning. Nevertheless, very few authors (Kulesza 1989, López and Terrada 1990; Congost Maestre 1994; Gutiérrez Rodilla 1998) analyse this phenomenon that in principle should not feature in medical language characteristics. The ideal situation should be that each specialised term has a unique meaning regardless of the context, in contrast with general language in which words may have several meanings depending on the context in which they appear (Kulesza 1989).
Polysemy usually appears in eponyms and in classical and Greco-Latin neologisms as a logical consequence of the lack of univocal meaning in their origins. Some examples of polysemy are síndrome de Cushing, Cushing’s syndrome or Cushing’s disease, or signo de Babinski, Babinski sign.
Synonymy is one frequent phenomenon in medical language, especially as far as eponyms, terms of classical origin and Greco-Latin neologisms are concerned. They come from the use of a wide series of root pairs, one of Greek origin and the other one of a Latin origin, that have the same meaning: nefropatía and renopatía; oftalmólogo and oculista, in Spanish or Cushing’s syndrome and Cushing’s disease, in English. In the same way, it is worth mentioning synonyms which come from the plurality of linguistic uses in diverse groups and geographical areas that try to overcome standardised nomenclatures. This phenomenon is more common in Spanish: trigonum femorale = triángulo de Scarpa, triángulo femoral, fosa de Scarpa.
There are also cases of quasi-synonyms. There are many concepts that can be referred to by several expressions that are, in principle, equivalent, but which are different depending on their point of view (anatomical, toponymic, historical or descriptive). Once again this phenomenon is more common in Spanish than in English. However, in the fourth section of this paper, we will analyse a particular case of synonyms in the English medical language (see below section 4).
Cerebral adiposity, Fröhlich’s syndrome = síndrome o distrofia adiposogenital, syndrome de Fröhlich, de Babinski-Fröhlich, de Laurence-Cleret.
Fold = pliegue, repliegue, fondo de saco, válvula, ligamento, surco, cresta.
Lymphoblastic erythroderma = linfodermia perniciosa, micosis fungoide, linfoblastoma cutáneo, reticulosis cutánea maligna.
Foreign words, borrowings and calques
This phenomenon is by far much more usual in English than in Spanish medical language. Some authors explain the phenomenon of foreign words (Latinisms, Anglicisms, Germanisms and Gallicisms), borrowings and calques, in other words, those phenomena derived from the influence of foreign languages, especially English (García Yebra 1988; Acosta 1988; Arrimadas 1988; Aleixandre et al. 1995; Navarro and Barnes 1996; Navarro 1997; Van Hoof 1999; González Pascual 2001).
There is an infinite list of Anglicisms in Spanish medical language which are commonly used because of their concision and brevity:
Test, widely used in Spanish instead of prueba, examen, análisis, ensayo.
Shock, instead of conmoción, impacto.
Rash, instead of erupción cutánea or sarpullido.
Stress, instead of estrés, tension nerviosa or psíquica.
Screening, instead of detección sistemática or cribado.
There is certain confusion when it comes to distinguishing the foreign word from the borrowing. Some authors consider that the borrowing has been adapted to the Spanish linguistic system, while the foreign word stays as it is (García Yebra 1988).
Still there are other authors who consider that the foreign word is a variant of borrowing, and one of the possible explanations for the penetration of the word in the Spanish language. Santoyo (1988) points out that borrowings are kept in the foreign language (foreign word) or are adapted graphically and phonologically, and Aleixandre et al. (1995) highlights that sometimes the foreign term is not copied word-for-word (foreign word) but is rather adapted with more or less modifications, as in randomización, which means distribución aleatoria, from the English word randomization or randomisation.
As for the calque, according to Van Hoof (1999) it is the translation of a borrowing, regardless of whether it consists of one or several elements. This author distinguishes between (1) «expression calques», which respect the syntax of the target language (hemolytic serum translated by suero hemolítico, when the Spanish word is suero hemolizado) (2) «structural calques», which introduce a less frequent construction in the target language, a frequently used calque in medical terminology, as serum globulin which is translated by seroglobulina, or signal sympton, síntoma guía, and (3) «false cognates» (anthrax translated by ántrax, when the correct Spanish word is carbunco).
Neologisms
Another quite frequent phenomenon in medical texts is neologisms (López are Terrada 1990; Arrimadas 1988; Ordóñez Gallego 1990; Gutiérrez Rodilla 1996; González Pascual 2001). According to Congost Maestre (1994), «neologisms» are new created words or existent words that have acquired a new meaning and which will last or disappear depending on the real necessities of their users. Neologisms can appear at different levels, as newly-coined words, recently created locutions, new collocations, compound nouns, new terminology, old words and locutions with new meanings, acronyms, abbreviations and eponyms.
Some examples of neologisms are hepatomegalia, from the English word hepatomegaly, or organomegalia, a literal translation of organomegaly, when in Spanish there is a more frequent word, visceromegalia.
Acronyms
Medical language is no exception to specialised languages as to the abusive use of acronyms. From a linguistic point of view, these phenomena replace the natural elements of a language, the words. From a scientific perspective, they are a most imprecise and dangerous instrument because they contradict the basic norms of scientific language, they do not belong to a system under established conventions, but rather are temporary and depend on the whim of the creator or editor. In addition we should mention the lack of international equivalence of compression phenomena.
Thus, they are the phenomena par excellence of medical language, and one of the most affected by the influence of the English language (López and Terrada 1990; Aleixandre et al. 1995; Gutiérrez Rodilla 1996; Van Hoof 1999: Martínez Odriozola 1999; González Pascual 2001). They are most difficult to translate, especially in those cases when the original meaning of the acronym has been forgotten, as in laser, which comes from the term light amplification by stimulated emission of radiation.
The phenomena of linguistic economy are more used in some medicine branches, especially in endocrinology, immunology or virology. In Spanish, they also appear frequently in medical records or referral notes: G3 P2 A1 C0 (3 gestaciones, 2 partos, 1 aborto, ninguna cesárea). The linguistic chaos is absolute when they are combined with mathematical signs: AC*FA (arritmia completa por fibrilación auricular) (Aleixandre et al. 1995).
With reference to the influence of English on Spanish medical language, Van Hoof (1999) categorises four different types of acronyms:
— When the acronym is identical in both languages:
adp, adenosi diphosphate = adp, adenosindifosfato
ecg, electrocardiogram = ecg, electrocardiograma
vd, respiratory dead space = vd, espacio muerto
— When the acronym is different in both languages:
dna (deoxyribonucleic acid) = adn (ácido desoxirribonucleico)
— When the acronym does not exist in Spanish:
acd, absolute cardiac dullness = zona de matidez cardíaca
ect, electric convulsive therapy = convulsiterapia, sismoterapia eléctrica
wbc, white blood count = recuento leucocitario
— When the acronym does not exist in English:
acute lung edema = eap, edema agudo de pulmón
intravenous urography = uiv, urografía intravenosa
In Spanish there are several translation problems as a result of an inadequate use of acronyms:
— When an acronym can be interpreted in a different way depending on the doctor’s speciality or the lack of international equivalence. For instance, in Spanish gea for a digestologist means gastroenteriris aguda, but for a nephrologist means glomerulonefritis extramembranosa aguda. Another example is em, which for the cardiologist means estenosis múltiple and for the neurologist is an esclerosis múltiple. Martínez Odriozola (1999) also denounces this problem and provides the following examples:
pcr = Polymerase Chain Reaction (microbiologist)
Proteína C reactiva (rhumatologist)
Parada cardiorrespiratoria (anesthetist)
rcp = Reanimación cardiopulmonar (anesthetist)
Reacción en cadena de la polimerasa (microbiologist)
em = Esclerosis múltiple (neurologist)
Estenosis mitral (cardiologist)
— When the same concept can be referred to by different acronyms, depending on the user’s preference. Bronquitis crónica: boci, bnco, epoc, ocfa, lcfa, bc.
— Considering the influence of the English language, in Spanish some authors tend to use the English acronyms while others use the Spanish ones, which causes a lack of standard terminology:
dna (deoxyribonucleic acid) = dna, while the proper term is adn (ácido desoxirribonucleico)
mhc (major histocompatibility complex) = mhc (complejo mayor de histocompatibilidad), very used in Spanish instead of cph (complejo principal de histocompatibilidad).
Eponyms
Without a doubt, the author who has studied medical eponyms most thoroughly is Van Hoof. This author created a classification of medical eponyms in 1986 which even nowadays is an invaluable tool for translators. It is worth mentioning the comparative analysis by Van Hoof (1999) between English and Spanish eponyms, which provides a most clear idea of the difficulties that the translation of eponyms entails.
Van Hoof lists several types of eponyms according to the influence of English in the Spanish language:
— Banalised eponyms, that is to say, those which have been used as a noun or as an adjective: bartolinitis, politzerización.
— Identical eponyms in English and Spanish:
Cushing’s síndrome = síndrome de Cushing
McBurney’s point = punto de Mac Burney o de Mc Burney
Ducts of Cuvier = conductos de Cuvier, seno de Cuvier
Ampulla of Vater = ampolla de Vater
— Identical compound eponyms in English and Spanish, which are named after two different authors:
Klippel-Feil’s síndrome = syndrome de Klippel-Feil
Ascheim-Zondeck test = prueba de Ascheim-Zondeck
— Identical double-eponyms but with a word order shift:
Jacob-Creutzfeldt disease = enfermedad de Creutzfeldt-Jacob.
— Identical eponyms but with different meanings:
Kirschner’s apparatus = agujas de Kirschner
Luschka’s crypts = glándulas de Luschka
Westphal-Plitz phenomenon = reflejo de Westphal-Plitz
— Identical eponyms but with a complementary precision of meaning:
· Complementary precision in English:
Cooper’s suspensory ligament = ligamento de Cooper
Loewenthal’s marginal bundle = fascículo de Löwenthal, fascículo tectospinal
· Complementary precision in Spanish:
Laënnec’s pearls = catarro pituitoso de Läennec
Welander’s ulcer = úlcera veneroide de Welander
· No equivalent eponym in Spanish:
Jacquet’s erythema = dermatitis del pañal
Malgaigne’s pads = panículo adiposo de la rodilla
· No equivalent eponym in English:
Tentorial nerve = nervio de Arnold
Main bundle = haz o fascículo de His
Straight-leg-raising test = signo de Lasègue
False cognates
False cognates represent another frequent characteristic of Spanish medical language based on the influence of English. Mayoral (1992) distinguishes between the following types of false cognates:
— Partial false cognates: there is a false cognate for one of the meanings and not for the other one, as in sinus = seno, trayecto.
— Crossed false cognates: pairs of terms in each language which presents false cognates for both meanings:
Fluorine = flúor
Fluor = fluorita
Anthrax = carbunco
Carbuncle = ántrax
— Paronyms or internal false cognates, which are those terms with a similar form but a quite different meaning. Normally they have different suffixes.
Canceroso (que tiene cáncer), cancerígeno (que produce el cáncer).
Cancerogenic (cancerígeno), cancerocidal (cancericida).
There are cases when false cognates exist given the diversity of terms with which a concept is used in different fields for one language and not for another language.
Eje = Axis.
Axis of symmetry (mathematics)
Axis of a lens (optics)
Axes (reference lines, crystallography)
Axle (technology)
Axis (botanic)
Axes (zoology)
Other examples are:
Blood pressure = tensión arterial
Bucca = mejilla
Columnar cell = célula cilíndrica
Communicable = contagioso
Contraceptive = anticonceptivo
Gland = ganglio, glándula
Gripe = cólico
Humanized milk = leche maternal
Hydrocarbon = hidrocarburo
3.3. Morphological and syntactic level
Within this level we also observe the influence of English in Spanish medical language.
Abuse of passives
Several authors have highlighted the abuse of passives as the most common syntactic feature in medical texts (Hernández et al. 1999; Gutiérrez Rodilla 1996; Van Hoof 1998; Rouleau 1993b). Some examples in English and Spanish would be:
The samples obtained from 16 randomly selected patients, monitored for up to 5 years, were studied by qualitative and semiquantitative rt-pcr-nah and by real-time rt-pcr to detect the hcv rna positive strand
The replicative hcv rna negative strand was examined in PBMC after culture with a T cell proliferation stimulating mitogen
In human cancer, a role has been suggested for the human polyomavirus bk
148 pacientes con infección por uhc, demostrada por la presencia de arn de uhc, fueron consecutivamente estudiados. Las células mononucleares de sangre periférica fueron marcadas con anticuerpos monoclonales y medidas por citometría de flujo
English is considered responsible for the abundance of passives in Spanish texts, for the Spanish language has a clear preference for active sentences and when it uses the passive voice it adopts the pronominal or reflexive form. Therefore, the passive voice is not typical of Spanish, firstly because languages for specific purposes were not invented in the second half of the 20th century, but rather evolved over 25 centuries. Before English, there were other predominant languages, classical and modern, but till the predominance of English passives were not so commonly used. Secondly, even Anglo-Saxons themselves criticise the exaggeration of passives in their proper language; and thirdly, their use does not turn the text into a more scientific document; on the contrary, when dissociating the semantic agent from the syntactic subject the text is less precise, which goes against one of the main characteristics of scientific language –accuracy.
Abuse of gerunds
Finally, the abuse of gerunds in Spanish medical language is another characteristic derived from the influence of English.
Evidence supporting a possible role for BKV in human cancer has accumulated slowly in recent years
The incidence and risk factors of malignancy were studied in 187 consecutive liver transplant recipients surviving more than 3 months
This study investigated breast and colorectal cancer screening among 196 low-income women being treated for psychiatric illnesses
La ILPR representa casi la tercera parte del total de ILP concedidas, siendo la artrosis su causa más frecuente
4 de los 39 pacientes presentaron un LNH, resultando en una prevalencia del 10%
Other morphological and syntactic phenomena
It is worth mentioning in this section the union by hyphens of affixes and nouns in order to create perfect compounds, which is also an influence of the English language. As a matter of fact, this language uses hyphened adjectives or nouns very frequently, but in Spanish this was not so common and goes against linguistic rules:
Anti-endothelial, translated in some cases into anti-endotelial, instead of antiendotelial).
Anti-inflammatory, translated sometimes into anti-inflamatorio, when in Spanish the proper word would be antinflamatorio, avoiding the repetition of the vowel i.
Antiulcer agents, translated in some cases into agents anti-ulcerosos, when the correct term would be agents antiulcerosos.
Another characteristic in which we can observe the influence of English are the mistakes when writing words that include the phoneme «r» in compound nouns. In these cases, the «r» is written instead of «rr», which would be the appropriate option:
Colorectal cancer, translated into cáncer colorectal, instead of cáncer colorrectal.
Radioresistance, translated into radioresistencia, instead of radiorresistencia.
4. differences and similarities between english and spanish medical languages
One of the most important and obvious similarities between English and Spanish medical languages is their Greco-Latin origin, which has endowed both languages with a certain terminological uniformity which currently only remains in the list of anatomical terms of the Nomina Anatomica, in the Index nominum genericorum plantarum and in the International Code of Nomenclature of Bacteria.
In both languages we can observe the influence of Greek and Latin in the creation of words. As a result, it is easier to translate the most erudite terms with a Greco-Latin base from English into Spanish, because the term remains practically invariable:
Cephalgia = cefalalgia (from the affix cefal, which means head).
Osteoarticular system = aparato osteoarticular (from the affix ost, which means bones).
Anodontia = anodoncia (from the suffix –ontia, which becomes –oncia in Spanish and which means teeth).
Nephrologist = nefrólogo (from the affix nephr, which means kidney).
Nevertheless, English terminology tends to be more descriptive and less «esoteric» (Van Hoof 1999) than the Spanish one, and popular terms are more frequently used. For this reason, English has a peculiarity which does not exist in Spanish: for a great deal of terms English has an erudite Greco-Latin term and a more popular name which is more common, however, in some cases it only has the popular term (Van Hoof 1990).
The origin of term-coupling can be found in English medical language history. Popular medical languages have always existed in the oral tradition in the regions absorbed by the Roman Empire. When it fell, Latin continued to be the only language for scientific communication all over Western Europe, which was exclusive in religious schools, but doctors communicated with people through vernacular English. Consequently, English has two terms for a concept: the erudite word (from a Greek or Latin root) and the vernacular one.
Spanish lacks this kind of term-coupling, and normally it only has an equivalent term for both English terms:
Coagulation (erudite), clotting (popular)= coagulación
Cicatrization (erudite), scarring (popular)= cicatrización
Lordosis (erudite), hollow back, saddle back (popular)= lordosis
Myopia (erudite), shortsightedness (popular)= myopia
Backalgia (erudite), back pain (popular) = raquilagia, dorsalgia.
The paradox is that the most erudite term is usually the most similar to the equivalent Spanish term, and for a doctor or translator it is more difficult to understand or to translate the popular term, in other words, the specialised is in this case the easiest.
Other differences between English and Spanish medical languages are:
— In those cases when Spanish has two synonymous terms, both words belong to a high register, in contrast to English which has a popular and an erudite term:
Xeroderma, paper skin = xerodermia, asteatosis
Niphablepsia = nifablepsia, ceguera de la nieve
Anarthria, jumbled speech = anartria, afasia motriz subcortical
— The derivation of adjectives is more erudite in Spanish than in English for Spanish uses suffixes, while English leaves the term just as it is:
Taste buds = papilas gustativas
Sweat gland = glándula sudorípara
Ball-and-socket joint = articulación orbicular, multiaxial, esferoidal
Pigment granules = gránulos pigmentarios
Rice bodies = cuerpos riciformes
Thus, when a Spanish adjective is translated into English, the translator turns to the popular term:
Lengua depapilada = bald tongue
Gota tofácea = chalky gout
Tics de Salam = nodding spasm
— Compound adjectives are very frequent in Spanish in contrast to English:
Basal cell carcinoma = epitelioma basocelular
End-to-side anastomosis = anastomosis lateroterminal
When translating from English into Spanish it is worth mentioning the translation strategies of modulation and transpositions. A transposition is a change of one part of the speech for another without changing the sense. Some examples of transpositions would be:
· Simple transposition:
skin graft = injerto cutáneo
apical pleurisy = pleuritis apical
sliding hernia = hernia por deslizamiento
· Crossed transposition:
Meralgia paresthetica = meralgia parestética
atonic bladder = atonía vesical
embolic pneumonia = embolia pulmonary
Bacterial offender = bacteria causal
Modulations are a variant of transpositions which consists in a change of the point of view and along with transpositions represents one of the most used strategies in translation (Van Hoof 1999). According to the typology of modulations, we have found the following examples:
· Concrete-abstract:
systemic circulation = circulación mayor (also circulación sistémica)
· Popular – erudite:
bad breath = halitosis
barber’s itch = sicosis de la barna, foliculitis de la barba
blood picture = hemograma
cough relieving = antitusivo
hip bone = hueso iliaco
stroke output = gasto sistólico
· Means-result:
needle biopsy = punción-biopsia
forced expiratory volume = volumen espiratorio máximo
· Cause – effect:
depot penicillin = penicilinas retardadas
· Whole-part:
mearus of nose = meato nasal
· Part – whole:
breast feeding = lactancia materna
· Part – another part:
billary colic = cólico hepático
mouth of uterus = cuello del útero
· Geographical:
Tashkent ulcer = botón de Oriente
· Symbol shift:
hay fever = fiebre del heno
iron lung = pulmón de acero
· Inversion of the point of view:
absent breath sounds = silencio respiratorio
missed labour = retención fetal
· Negation of opposite:
analgesics are supposed to be non addictive = se supone que los analgésicos no crean adicción
5. conclusions
In this paper we have described the characteristics of the Spanish medical language in contrast to English medical language for this language is nowadays the lingua franca of the international medical community. Given the fact that a high percentage of medical publications and conferences are in English, medicine represents a most interesting field for translators whose language combination is English-Spanish. We consider that in order to achieve a high quality translation, translators must be aware of the characteristics of medical language and must take into account the changes and the evolution of medical language since the irruption of English into the international medical scene. The knowledge of these changes and features will lead the translators to choose the translation strategies and procedures in accordance with the use of terms in one language or another.
The analysis of the current Spanish medical language has shown, on the one hand, that the translations of new terms or the development of other terms are not always satisfactory for they almost always contradict the ideal characteristics of scientific language, namely accuracy, univocity of meaning and clarity. On the other hand, we have learned that Spanish medical language does not always respect the linguistic norms system. However, we must bear in mind that the translator is a means of communication, thus the ultimate target is to achieve communication between two interlocutors. In order to do this, sometimes it is more important to adapt the discourse to the final user than to pursue a linguistic purism that sometimes jeopardises this communication.
Finally we subscribe the words of Barber (1992) who underlines that the hegemony of English is the consequence of the «onrush of economic and ecological forces that demand integration and uniformity and that mesmerize the world with fast music, fast computers, and fast food with MTV, Macintosh, and McDonald´s, pressing nations into one commercially homogeneous global network». According to this author, globalization not only applies to technology and commerce, but also to communication and language, to international discourse, and hence to translation.
recibido en febrero 2007
aceptado en octubre 2007
6. bibliography
Acosta, L. A. (1988). «Transferencias lingüísticas: préstamos y calcos». AA.VV. Problemas de la traducción, pp. 51-57.
AA.VV (eds.) (1988). Problemas de la traducción. Madrid: Fundación Alfonso X El Sabio.
Aleixandre, R., Porcel, A., Agulló, A. y Marset, S. (1995). «Vicios del lenguaje médico (I). Extranjerismos y acrónimos». Atención Primaria 15 (2), pp. 113-117.
Ángel Mejía, G. (2005). Diccionario de laboratorio aplicado a la clínica. Bogotá: Editorial Médica Panamericana.
Arntz, R., Picht, H. (1995). Introducción a la terminología. Madrid: Fundación Germán Sánchez Ruipérez.
Arrimadas Saavedra, J. (1988). «Préstamos, barbarismos y neologismos en la traducción científica y técnica». IN: AA.VV. (1988), pp. 59-73.
Barber, B. (1992). «Jihad vs. McWorld». The Atlantic Monthly 3, pp.53-63.
Cabré, T. (1993). La terminología. Teoría, metodología, aplicaciones. Barcelona : Antártida.
— (2002). «Análisis textual y terminología, factores de activación de la competencia cognitiva en la traducción». Alcina, A., Gamero, S. (eds.). La traducción científico-técnica y la terminología en la sociedad de la información. Castellón de la Plana: Publicacions de la Universitat Jaume I.
Congost Maestre, N. (1994). Problemas de la Traducción Técnica: Los Textos Médicos en Inglés. Alicante: Universidad.
DORLAND’S Illustrated Medical Dictionary, 28th ed (1994). Philadelfia: WB Saunders Co.
Felber, H. & Picht, H. (1984). Métodos de terminografía y principios de investigación terminológica. Madrid: Instituto Miguel de Cervantes/CSIC.
Fishbach, H. (1986). «Some anatomical and physiological aspects of medical translation». Meta, March, pp. 16-21.
— (1993). «Translation, the great pollinator of science: a brief flashback on medical translation». Babel, 38 (4), pp. 193-202.
Gancedo, C. (1994). «¿Tú bloteas o transfieres?». Boletín de la Sociedad Española de Bioquímica y Biología Molecular 114.
García Yebra, V. (1988). «Préstamo y calco en español y alemán. Su interés lingüístico y su tratamiento en la traducción». AA.VV. Problemas de la traducción, pp. 75-90.
González Pascual, A.L. (2001). «Defectos gramaticales y de estructuración literaria más frecuentes. Uso de términos incorrectos». Medicina Clínica 35, pp. 131-134.
Gutiérrez Rodilla, B.M. (1996). «El lenguaje médico, un enfermo no imaginario». El Médico, 15 de marzo.
— (1997). «La influencia del inglés sobre nuestro lenguaje médico». Medicina Clínica 108, pp. 307-313.
Hoffman, L. (1979). «Towards a theory of LSP. Elements of a methodology of LSP analysis». Fachsprache 79(1-2), pp. 12-17.
Jiménez, O. (2002). La traducción técnica inglés-español. Didáctica y mundo profesional. Granada: Comares.
Kulesza, K. (1989). «Some thoughts on various approaches to a definition of LSP». Unesco-Alsed-LSP Newsletter 11 (2), pp. 34-37.
Lerat, P. (1997). Las lenguas especializadas [traducción de A. Ribas de Les langues spécialisées (1995)]. Barcelona: Ariel.
López, J.M., Terrada, M.L. (1990). Introducción a la terminología médica. Barcelona: Salvat Editores.
Martínez Odriozola, P. (1999). «Abuso de las siglas en el lenguaje médico: ¿PCR o RCP?». Medicina Clínica 58, 640, pp. 375 – 376.
Masson (1992). Diccionario terminológico de ciencias médicas. Barcelona: Masson S.A.
Mayoral, R. (1992). «Los falsos amigos en la traducción de textos». V Congreso de Farmacéuticos Ibero-Latinoamericanos «La Farmacia del ayer, la Farmacia de hoy y la Farmacia del futuro». Alicante.
Munday, J. (2002). Introducing translation studies. London: Routledge.
Navarro, F.A. (1997). Traducción y lenguaje en medicina. Barcelona: Fundación Dr. Antonio Esteve.
─ (2002). «La traducción médica ante el siglo XXI: tres retos para el lenguaje científico en español». IN: <http://www.el-castellano.com/fnavarro.html>.
─ (2005). Diccionario crítico de dudas inglés-español de medicina. McGraw Hill. Interamericana de España, S.A.
Navarro, F. A., Barnes, J. (1996). «Traducción de títulos al inglés en Medicina Clínica: calidad e influencia del castellano». Medicina Clínica 106 (8), pp. 298-303.
Ordóñez Gallego, A. (1990). «Algunos barbarismos del lenguaje médico». Medicina Clínica 94, pp. 381-383.
Pilegaard, M. (1997). «Translation of medical research articles». IN: Trosborg, A. Text typology and translation. Amsterdam-Philadelphia. John Benjamins, pp. 159-184.
Rodríguez Díez, B. (1979). «Lo específico de los lenguajes científico-técnicos». Archivum 27-28, pp. 485-521.
Rouleau, M. (1993). «Des traquenards de la versión médicale. I. Action, effect, potency et effectiveness». Meta 38, pp. 268-274.
Sager, J. C. (1993). Curso práctico sobre el procesamiento de la terminología. Madrid: Fundación Germán Sánchez Ruipérez.
Santoyo, J.C. (1988). «Los calcos como forma de traducción». IN: AA.VV. Problemas de la traducción. pp. 91-97.
Segura Munguía, S. (2004). Diccionario etimológico de medicina. Bilbao: Universidad de Deusto.
Sliosberg, A., M.D. (1971). «Quelques considerations sur la traduction médicale et pharmaceutique». Babel 17 (1). pp. 21.
Snell-Hornby, M. (2006). Turns of Translation Studies: New Paradigms or Shifting Viewpoints? Philadelphia, PA, USA: John Benjamins Publishing Company.
Stedman (2001). Diccionario bilingüe diccionario de ciencias médicas : inglés-español, español-inglés. Buenos Aires: Editorial Médica Panamericana.
Van Hoof, H. (1999). Manual práctico de traducción médica. Diccionario básico de términos médicos (inglés-francés-español). Granada: Comares.
Yetano Laguna, J., Alberola Cuñat, V. (2003). Diccionario de siglas m édicas y otras abreviaturas, epónimos y términos médicos relacionados con la codificación de las altas hospitalarias. Madrid: Ministerio de Sanidad y Consumo.