Descriptive Statistics and Bivariate Correlations among Variables in the Study (N = 955)
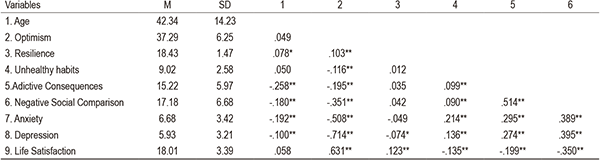
* p ≤ .05, ** p ≤ .01
Many ways of facing an extreme event: Profiling of different coping groups during the COVID-19
Diferentes formas de enfrentar una situación extrema: Perfiles de afrontamiento durante el confinamiento por COVID-19
Covadonga González-Nuevo1, Álvaro Menéndez-Aller1, Álvaro Postigo1, Jaime García-Fernández1, Eduardo García-Cueto1, Marcelino Cuesta1 and José Muñiz2
1Universidad de Oviedo
2Universidad Nebrija
ABSTRACT
Background. Numerous studies have examined the consequences of the COVID-19 lockdown on mental health. Nonetheless, there is no comprehensive analysis of different profiles of coping strategies based on relevant sociodemographic characteristics (gender, age and decreased income), maladaptive habits during lockdown (level of problematic use of social networks and unhealthy habits), and protective personality variables (resilience and optimism). Method. 1003 participants (75.5% women), aged 18-83 years (M = 42.33; SD = 14.32) completed an online questionnaire. A cluster analysis identified the different groups in the sample using variables of problematic social network use, unhealthy habits, gender, age, decreased income, resilience and optimism. Differences between the various groups were subsequently analysed using various ANOVAs. Results. Four coping groups were identified, labelled Young Optimists, Young Pessimists, Middle-aged Optimists and Resilient Elders, with significant differences between them in all of the study variables. Conclusions. This study identified fundamental characteristics of different coping groups during the COVID-19 lockdown. This result allows us to identify which behaviours and traits characterize the most-affected individuals.
Keywords: cluster, optimism, resilience, COVID-19, problematic social networking use
RESUMEN
Antecedentes. Existen múltiples estudios que analizan las consecuencias del confinamiento para la salud mental. No obstante, no existen estudios que analicen los diferentes perfiles de afrontamiento de la situación dependiendo de características sociodemográficas relevantes (sexo, edad y pérdida de ingresos), de los hábitos desadaptativos llevados a cabo durante el confinamiento (nivel de uso problemático de Redes Sociales y hábitos no saludables), y de variables de personalidad protectoras (resiliencia y optimismo). Método. 1003 participantes (75.5% mujeres), con un rango de edad entre 18 y 83 años (M = 42.33; SD = 14.32) contestaron un cuestionario online. Se realiza un análisis de clúster para identificar los diferentes grupos en la muestra dependiendo de las variables de uso problemático de redes sociales, de hábitos no saludables, sexo, edad, pérdida de ingresos, resiliencia y optimismo, tras ello se analizan las diferencias entre los diversos grupos mediante varios ANOVAs. Resultados. Existen cuatro grupos de afrontamiento denominados Jóvenes Optimistas, Jóvenes Pesimistas, Personas de Mediana edad Optimistas y Personas de Mayor Edad Resilientes con diferentes significativas entre ellos en ansiedad, depresión e insatisfacción con la vida. Conclusiones. Este estudio permite conocer las características fundamentales de los diferentes grupos de afrontamiento durante el confinamiento.
Palabras Clave: clúster, optimismo, resiliencia, COVID-19, uso problemático de redes sociales
Cite as: González-Nuevo, C., Menéndez-Aller, A., Postigo, A., García-Fernández, J., García-Cueto, E. Cuesta, M., & Muñiz, J. (2023). Many ways of facing an extreme event: Profiling of different coping groups during the COVID-19. Escritos de Psicología – Psychological Writings, 16(2), 91-103. https://doi.org/10.24310/escpsi.16.2.2023.14848
Corresponding author: Covadonga González-Nuevo. Department of Psychology. Universidad de Oviedo. Plaza Feijoo s/n 3303 Oviedo (Spain). Email: covadongagonz@gmail.com
INTRODUCCIÓN
On March 16, 2020, Spain declared a state of alarm due to a large number of people infected by COVID-19 and the rapid spread of the virus, resulting in the population being confined. The mental health of the population has been an object of study since the lockdown. Spain’s rates of depression and anxiety reached between 20 and 30% (González-Sanguino et al., 2020; Gutiérrez-Hernández et al. 2021; Sandín et al., 2020; Valiente et al., 2021), numbers similar to other countries (Kira et al., 2021; Salari et al., 2020). There were also reports of increased life dissatisfaction (Cong, 2021; Li et al., 2020; López-Núñez et al., 2021), defined as the subjective evaluation of one’s current quality of life, which is an essential indicator of psychological health and well-being (Li et al., 2020). Different variables related to poorer mental health in isolation have been identified, such as being young, female, experiencing a fall in income (González-Sanguino et al., 2020), unemployment during isolation, and looking after children (Gutiérrez-Hernández et al., 2021).
Within this context of generalized stress during isolation, there were different levels of impact on mental health as well as different ways of coping with the situation. The population’s habits need to be identified in order to better understand its coping strategies. In this regard, it is worth noting the increased use of legal substances such as alcohol (Calina et al., 2021), tobacco (Stanton et al., 2020; Valiente et al., 2021) or anxiolytics and hypnotics, with the latter especially in older people (García-Fernández et al., 2020). There was also a notable increase in the use of illegal substances such as marijuana (Solé et al., 2021) and other illicit drugs such as cocaine and methamphetamines (Been et al., 2021), with fear of COVID-19 being one of the main reasons for consumption (Rogers et al., 2020).
The lockdown also changed social interaction. Social Networking Sites (SNS) became the only way of communicating, and saw a massive increase in their use (Vall-Roqué et al., 2020). This increased use might have led to a rise in problematic use of SNS (Cudo et al., 2020). Problematic SNS use is characterized by excessive preoccupation, strong motivation to use SNS, and spending so much time and effort on it that it negatively affects other social activities, study or work, interpersonal relationships, and psychological health and well-being (Andreassen & Pallesen, 2014) excessive, and compulsive social network activity has increased the last years, in which terms such as ”social network site addiction\” and \”Facebook addiction\” have been used interchangeably. The aim of this review is to offer more knowledge and better understanding of SNS addiction. There are various problematic SNS behaviours with negative mental health consequences: negative comparative use and addictive consequences (González-Nuevo et al., 2023). Comparative use is defined as the tendency to compare oneself to others by feeling inferior and has been linked to adverse effects on well-being both before (Balaban & Spoaller, 2020; Brailovskaia et al., 2021) and during lockdown (González-Nuevo et al., 2022). Addictive use has been related to negative mental health consequences both before (Boursier, et al., 2020) and during the lockdown (González-Nuevo et al., 2022; Haddad et al., 2021).
Finally, given the negative effects that excessive use of SNS in isolation can have on mental health, it is important to determine which protective psychological variables can reduce these effects. Resilience stands out as a variable protecting the population from psychological distress (Osofsky & Osofsky, 2013). It is defined as the process of adapting well to adversity, trauma, tragedy, threats or significant sources of stress (APA, 2014). In the Spanish context of isolation, being male, being older and being more physically active were protective factors against psychological distress (Carriedo et al., 2020). The same factors have also been associated with lower fear of COVID and higher life satisfaction (Gundogan, 2021), as well as lower levels of depression (Verdolini et al., 2021) and anxiety (Liu et al., 2020; Pérez-Rojo et al., 2021). Optimism is another important variable that has also been found to be related to better coping with stressful situations (Baumgartner et al., 2018). Optimism is defined as the tendency to think that favourable events will happen even when facing obstacles (Carver et al., 2010). Optimism has been related to lower emotional distress in lockdown (Gori et al., 2020; Sica et al., 2021) with no significant differences between sexes (Koliouli & Canellopoulos, 2021).
To date, studies on mental health in lockdown have only provided prevalence of different measures of emotional distress and life satisfaction and their relationship with risk and protective variables, which is not comprehensive information. In an attempt to present a more thorough approach, this paper will try to describe the different coping groups in an extreme situation, the COVID-19 lockdown. To this end, we will combine information about the most important socio-demographic characteristics at this critical moment, such as age, sex and loss of income. This will allow us to determine the socio-demographic characteristics identifying each group. This information will also be combined with maladaptive coping behaviours such as problematic SNS use (both addictive and comparative), unhealthy behaviours, and protective personality traits such as resilience and optimism. Hence, for each group we will have socio-demographic information, maladaptive coping habits and protective personality traits, providing very interesting preventive information. Although no previous studies have combined these variables, given previous research, we can expect a negative relationship between age and problematic SNS use, as well as between problematic SNS use and optimism and resilience. Similarly, unhealthy habits are expected to be related to lower resilience and optimism.
The general aim of this study is to analyse whether there were different coping strategy groups during lockdown and if so, to characterize the emotional distress and life dissatisfaction these groups experienced. This general objective is broken down into three specific goals: (i) to determine whether various coping strategy groups exist based on maladaptive behaviours during lockdown (level of problematic SNS use and unhealthy habits), relevant socio-demographic variables (age, gender and decreased income) and coping resources (resilience and optimism); (ii) to detect any differences between the coping strategy groups in terms of levels of anxiety, depression, and life satisfaction; and (iii) to describe the sociodemographic characteristics of these groups.
METHOD
Participants
Sampling was done using a snowball procedure via SNS. The inclusion criteria were being over 18 and Spanish. Data were collected during the Spanish lockdown period between April 28 and May 6, 2020. A sample of 1,059 Spanish participants was initially obtained. Subsequently, 5.29% were removed because they did not satisfy the attentional criteria, i.e., two or more incorrect responses on the attentional control scale. The final sample was therefore made up of 1,003 participants (75.5% women), aged 18-83 years (M = 42.33; SD = 14.32).
Instruments
Problematic Use of SNs questionnaire (PUS; González-Nuevo et al., 2023)
This is a self-report made up of 18 Likert-type items divided into two scales addressing problematic use of social networks. The first scale, called addictive consequences, has 10 items and assesses the addictive use of social networks. The second scale, negative social comparison, has 8 items and measures the degree to which respondents use social networks to compare themselves with others, believing themselves to be inferior. All items have five response options, where 1 indicates “strongly disagree” and 5 indicates “strongly agree”. In the present study, the internal consistency of the negative social comparison and addictive consequences scale were excellent (α = .94 and α = .91, respectively).
Satisfaction with Life Scale (SWLS; Diener et al., 1985)
The study used the Spanish adaptation of Vázquez et al. (2013). This is a self-report made up of 5 Likert-type items measuring the degree of satisfaction with life (i.e. “If I could live my life over again, I would change almost nothing”). All items have five response options, where one indicates “strongly disagree” and five indicates “strongly agree”. In the present study, the internal consistency of the scale was good (α = .82).
Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983)
The Spanish adaptation from Terol et al. (2007) was used. This is a questionnaire consisting of 14 Likert-type items in two subscales each with 7 items. The first subscale, HADS_A, assesses the level of anxiety (i. e. “ Worrying thoughts go through my mind”). The second subscale, HADS_D, assesses the level of depression (i. e. “I feel as if I am slowed down”). All items are scored from 0 to 3, with higher scores indicating greater symptom severity. For both scales, the authors suggest that scores above eleven would indicate a “clinical case” and above eight would be considered a “probable case”. In the present study, the internal consistency of both scales was good (α = .84 for HADS_A and α = .77 for HADS_D).
Brief Resilience Scale (BRS; Smith et al.., 2008)
Specifically, the study used the Spanish adaptation (Rodríguez-Rey et al., 2016). This is an instrument with 6 Likert-type items aimed at assessing resilience—understood as the ability to recover from adversity and stress (i. e. “I do not take long to recover after a stressful situation”). All items have five response options, with 1 meaning “strongly disagree” and 5 meaning “strongly agree”. The internal consistency of the scale in the present study was good (α = .85).
Optimism subscale from the Entrepreneurial Personality Assessment Battery (BEPE; Cuesta et al., 2018)
The scale consists of 10 Likert-type items with five response alternatives, where 1 indicates “strongly disagree” and 5, “strongly agree” (i. e. “I think everything will be fine”). The consistency of the scale in the present study was excellent (α = .92).
Unhealthy habits questionnaire
This is a questionnaire with 7 items, created for this study, to assess engagement in unhealthy habits. The questions ask about increased consumption of alcohol, tobacco, cannabis, drugs (cocaine, crack, amphetamines, ecstasy, non-prescription opiates, or other drugs), anxiolytics and hypnotics during the lockdown (i. e. “My alcohol consumption has increased during the lockdown”). An item about self-harm during the lockdown was also included (i. e. “I have voluntarily self-harmed during lockdown”). The internal consistency of the scale was α = .62.
Data about socioeconomic status and health with regard to COVID-19 effects
The following data were collected: i) the number of cohabitants (possible answers: one, two, three, four or more); ii) employment status (unemployed before lockdown, unemployed since lockdown, in-person worker, remote-worker, or retired), iii) whether income had risen or fallen due to lockdown; iv) whether they were caregivers for minors or elderly dependents; v) whether or not they had relatives who were infected with COVID-19; and vi) whether they had relatives who died from COVID-19.
Attentional control scale
An attentional scale was used to check that respondents read the items carefully. This scale had 10 items, each with five options. Each item asked the respondent to choose a specific response (i. e. “Please select option 1”). These items were mixed in with the other scales and scored as correct or incorrect depending on the option selected.
Procedure
To administer the test, all of the instruments were combined in an online form in Google forms, links to which were shared through SNS. The items were randomly distributed in the questionnaire as recommended by research (Şahin, 2021; Weinberg et al., 2018), with the only criterion being that two items in a row were not measuring the same dimension.
At the beginning of the form, participants were informed that their data would be processed anonymously and purely for purposes related to the present study. Their informed consent was also requested before they could start answering.
The study was not explicitly reviewed by an Ethics Committee, given that this is not required by the University of Oviedo, nor by the national guidelines established in the Code of Ethics of the Spanish Psychological Association. There are several reasons why an explicit approval by an Ethics Committee was not necessary: the participants were adults, the evaluation was voluntarily accepted—implicit informed consent is assumed, and the data is treated anonymously and confidentially. In addition, all the recommendations established in ISO-10667 Standard for the evaluation of people were strictly followed. The whole evaluation process and the use of the measuring instruments followed the Deontological Code of the Spanish Psychological Association (2010), as well as the International Test Commission Guidelines for Test Use (2013).
Data Analysis
In order to identify the possible groups of participants, cluster analysis techniques were applied based on sex, age, decreased income due to the COVID-19 pandemic, and the scores for addictive consequences, optimism, resilience, negative social comparison and unhealthy habits. First, all variables were standardized and converted into Z-scores before the cluster analyses. Then, a hierarchical procedure was performed following the farthest neighbour method, using the squared Euclidean distance as a measure of proximity. The Dendrogram was used to determine the number of clusters to be retained. Subsequently, a non-hierarchical procedure (k-means) was followed to obtain the final grouping of subjects.
Before analysing differences between clusters in psychological variables (such as depression, Anxiety and Life Satisfaction), the data were tested for adherence to the assumption of homoscedasticity using Levene’s statistic. Although all variables demonstrated heteroscedasticity, we proceeded with a one-factor Analysis of Variance because it is robust to such violations (Blanca et al., 2017). We used partial eta squared to calculate effect size, such that values from .010 to .039 are considered a small effect, from .040 to .110, a moderate effect, and from .111 to .200, a large effect (Lenhard and Lenhard, 2016). Where statistically significant differences were observed, the Games-Howell post-hoc test was used to determine which groups the differences were between.
We used descriptive statistics to analyse the sociodemographic profile of each cluster. The mean and standard deviation were calculated for quantitative variables. For qualitative variables, the percentage of responses to each of the options within each cluster was obtained. The data were analysed with IBM SPSS (Version 24), with a confidence level of 95%.
RESULTS
Firstly, correlational analyses were conducted for all quantitative variables involved. A significant positive correlation was found between age and resilience and there was a negative correlation between age and problematic SNS use (both addictive and comparative). There was also a negative correlation of optimism with unhealthy habits and problematic SNS use (both addictive and comparative). However, the relationship between resilience and unhealthy habits and problematic SNS use (both addictive and comparative) was not significant. Finally, unhealthy habits and problematic SNS use were positively correlated. All results are shown in Table 1.
Table 1
Descriptive Statistics and Bivariate Correlations among Variables in the Study (N = 955)
* p ≤ .05, ** p ≤ .01
Subsequently, an exploratory hierarchical cluster analysis was carried out using sex, age, and decreased income during the COVID-19 pandemic and the scores from the addictive consequences, optimism, resilience, negative social comparison and unhealthy habits scales (standardized scores). A total of 48 subjects were removed for having extreme scores (three standard deviations above or below the mean), thus reducing the sample to 955 participants. Additionally, a Dendrogram was used to decide the number of clusters. Non-hierarchical cluster analysis (k-means) was performed based on the results, producing a four-group solution.
Table 2 shows the results of this analysis and the means and percentages of the variables used to form the clusters. Figure 1 contains a bar graph with each group’s typical mean scores in each of the quantitative variables that describe them. There are two coping groups, called Young Optimists and Young Pessimists, among young people with a very similar average age of around 28 years old. The Young Optimists is made up of young people with an above-average level of optimism, below-average problematic SNS use and unhealthy habits, as well as a lower percentage of participants with decreased income than the Young Pessimists group. On the other hand, the Young Pessimists are the young people with the lowest levels of optimism, the highest problematic SNS use and the highest levels of unhealthy habits compared to the rest of the groups, as well as having the highest percentage of participants with decreased income.
Two further clusters of older people are Middle-aged Optimists and Resilient Elders. The Middle-aged Optimists have an above-average level of optimism (albeit lower than the Young Optimists) and below-average levels of problematic SNS use and unhealthy habits. In addition, the percentage of participants with decreased income is very similar to the Young Optimists group. Finally, the Resilient Elders group is the oldest group (average age is around 62), with a lower percentage of women, a lower percentage of people with a decreased income, and below-average levels of problematic use of social networks and unhealthy habits. On the other hand, they have the highest level of resilience of the four groups.
Table 2
Cluster Analysis of k-means and Description of each Cluster in % of Women, % of People that Experienced a Decrease on Income and Age, Resilience, Optimism, Addictive Consequences, Negative Social Comparison and Unhealthy Habits Means (N = 955)
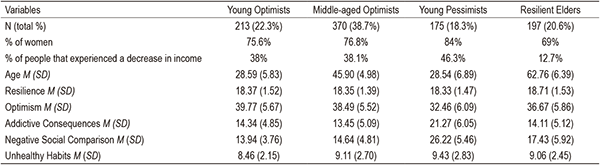
Figure 1
Profiles on Age, Negative Social Comparison, Addictive Consequences, Unhealthy Habits, Optimism and Resilience of the Clusters (N = 955)
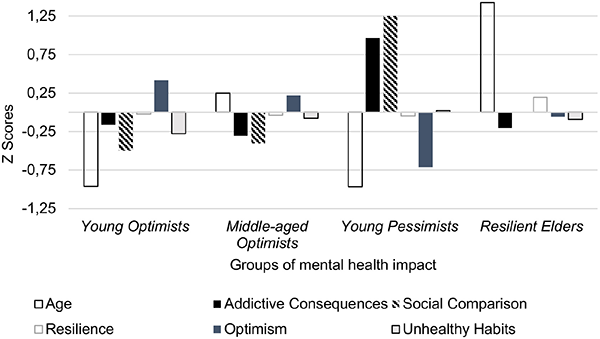
Table 3 shows the ANOVA results, as well as the effect sizes, the means of each group and the results of the post-hoc tests. Before examining which groups the differences were found between, the assumption of homoscedasticity was tested for compliance with Levene’s statistic. For all variables the null hypothesis was rejected at 95% confidence and, therefore, different variances are assumed. Hence, we proceeded with the Games-Howell test for all variables. As Table 3 shows, there were significant differences between the different clusters for the variables anxiety (F3,951 = 58.89, p < .001, η² = .157), depression (F3,951 = 50.56, p < .001, η² = .138) and life satisfaction (F3,951 = 39.96, p < .001, η² = .104). The effect size was large for anxiety and depression, and moderate for life satisfaction. The post-hoc test showed that differences were mostly found between the Young Pessimists group and the other clusters.
In particular, the Young Pessimists group had significantly higher levels of depression than the other groups. The Resilient Elders group were the second most depressed group—values for depression in the Resilient Elders group were significantly higher than the Young Optimists group and the Middle-Aged Optimists group. In terms of anxiety, it was again the Young Pessimists who exhibited significantly higher values than the other groups. Finally, life satisfaction was significantly lower for the Young Pessimists than the other groups. The next lowest life satisfaction was in the Resilient Elders.
Table 3
One-way ANOVA between Clusters, Effect Size, Variable Means and Games-Howell post-hoc test (N = 955)

Note. a: Young Optimists; b: Middle-aged optimists; c: Young Pessimists; d: Resilient Elders
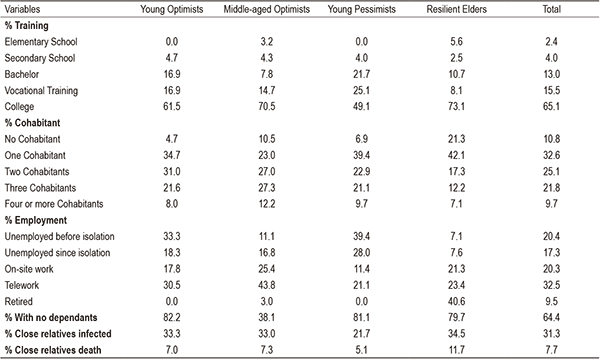
Lastly, Table 4 provides the sociodemographic characteristics of the different groups. The highest percentage of people who completed university education (73.1%) was in the Resilient Elders group. The Resilient Elders also had the highest percentage of people not cohabiting (21.3%) or with one cohabitant (42.1%). The percentages of people who lived with two cohabitants were similar in the Young Optimists (31%), Middle-aged Optimists (27%) and Young Pessimists (22.9%) groups. Finally, the Middle-aged Optimists had the highest percentage of people with three cohabitants (27.3%) and four or more cohabitants (12.2%). Looking at employment, it is worth noting that the highest percentage of unemployed people both during (28%) and before the lockdown (39.4%) was in the Young Pessimists, while the highest percentage of employed people who kept their jobs either in-person (25.4%) or remotely (43.8%) was in the Middle-aged Optimists. Finally, the Middle-aged Optimists group had the highest proportion of people who had to care for dependents (38.1% with no dependents). The Young Pessimistic Group had the lowest percentage of relatives who had been infected with (21.7%) or died from (5.1%) COVID-19.
Table 4
Clusters’ Sociodemographic Profile (N = 955)
DISCUSSION
The objective of our study was to explore whether there were different coping groups during the lockdown and if so, to characterize the emotional distress and life dissatisfaction experienced by these groups. This main objective produced three specific objectives: (i) to determine whether there were different coping groups depending on maladaptive behaviours during lockdown (level of problematic SNS use and unhealthy habits), relevant socio-demographic variables (age, gender and decreased income) and coping resources (resilience and optimism); (ii) to detect differences in levels of anxiety, depression, and satisfaction with life; and (iii) to describe the sociodemographic characteristics of these groups.
Based on the cluster analysis, we were able to distinguish four coping groups: 1) the Young Optimists, characterized by being the youngest, having the lowest levels of unhealthy habits and problematic SNS use, and the highest levels of optimism; 2) Young Pessimists, a group made up of young people with low levels of optimism, high levels of unhealthy habits, problematic SNS use, and a higher percentage of participants with decreased income; 3) Middle-aged Optimists, a group characterised by an average age of approximately 45, with low levels of problematic SNS use and unhealthy habits, and a high level of optimism, and 4) the Resilient Elders, which was the oldest age group, with lower levels of optimism than the other groups but slightly higher than average levels of resilience, low levels of problematic SNS use, and low levels of unhealthy habits. As in other studies, higher levels of optimism were related to lower levels of problematic SNS use (Liu et al., 2017) and lower levels of unhealthy habits (Nguyen, 2022; Singleton et al., 2022). On the other hand, being younger was related to higher levels of addictive and comparative problematic SNS use (Sechi et al., 2021; Yesilyurt & Turhan, 2020) and higher levels of depressive symptomatology and suicidal ideation during the lockdown (Urdiales-Claros & Sánchez-Álvarez, 2021). Previous studies have also found poorer mental health at lower income levels (Codagnone et al., 2020; González-Sanguino et al., 2020). However, we found no studies analysing the coping groups that can be extracted from all these variables together.
Among the groups we found, the differences between the two young groups were notable, with contrasting scores for problematic SNS use, unhealthy habits and levels of optimism. The fact that these two groups with such different coping behaviours existed at the same age highlights the need to identify this group of Young Pessimists in order to prevent them from engaging in maladaptive behaviours and to improve their protective variables. On the other hand, identifying the profile of the Young Optimists group and examining their coping strategies and characteristics will produce useful information for helping other young people cope better. One notable difference between these two groups was the decreased income, which was greater in the Young Pessimists than in the Young Optimists. Previous research has shown that decreased income is related to poorer mental health (Codagnone et al., 2020; González-Sanguino et al., 2020). Therefore, one direction for future research could be to find out if loss of income is the trigger for these maladaptive online and offline behaviours.
Looking at the older age groups, the Middle-aged Optimists exhibited a similar pattern to the Young Optimists—they had high levels of optimism and showed low levels of unhealthy habits and problematic SNS use. On the other hand, the Resilient Elders showed the most divergent pattern. This group was characterised by a below-average level of optimism and a higher level of resilience. This finding may seem contradictory at first glance as optimism and resilience were positively correlated and both have been considered protective variables for mental health during lockdown (Vos et al., 2021). We might therefore expect high levels of resilience to be related to high levels of optimism and better mental health. In this case, however, optimism was low and mental health was worse than average despite high resilience. One possible explanation for the lower-than-average optimism in this group is the objective risk of severe COVID-19 illness in the elderly during the lockdown (Lee et al., 2020). And although resilience did not lower the level of emotional distress to below the average, it did exhibit some protection, as the level of emotional distress was lower in the Resilient Elders than in the Young Pessimists. Future studies should clarify whether the protective power of resilience is greater in a less extreme situation than a lockdown in this particular age group. Furthermore, as expected given their older age, they had low levels of problematic SNS use. Previous studies have found this negative association between age and problematic SNS use (Sechi et al., 2021; Yesilyurt & Turhan, 2020). This group also did not have high levels of unhealthy habits. This finding highlights the need to know whether optimism and resilience protect differently depending on a person’s stage in life.
The coping groups we identified showed different levels of anxiety, depression and life satisfaction. In particular, the Young Pessimists was the group with the highest levels of depression and anxiety and the lowest levels of life satisfaction compared to the other groups. The next highest levels of depression and anxiety were in the Resilient Elders, who also had the second lowest levels of life satisfaction. The fact that the Young Pessimists group was characterised by low optimism and had poorer mental health is consistent with previous studies (Carriedo et al., 2020; Gori et al., 2020; Sica et al., 2021). This finding is consistent with previous evidence linking an increase in psychological distress to an increase in unhealthy habits (Calina et al., 2021; Stanton et al., 2020; Valiente et al., 2021; García-Fernández et al., 2020; Been et al., 2021) and with problematic SNS use (Keles et al., 2020; Balaban & Spoaller, 2020; Boursier, et al., 2020; Brailovskaia et al., 2021). It is notable that the Resilient Elders group, despite their above-average resilience, had poorer mental health than the other “optimistic” groups (Young Optimists and Middle-aged Optimists). This finding is inconsistent with previous studies claiming that a higher level of resilience would protect against poorer mental health (Osofsky & Osofsky, 2013). This group also did not engage in unhealthy habits and did not have a high percentage of economic losses related to poorer mental health (Codagnone et al., 2020; González-Sanguino et al., 2020; Sechi et al., 2021). However, one possible hypothesis for the high levels of psychological distress in this group may lie in the particularly dangerous situation they experienced during this period, when COVID-19 was a threat to their health (Lee et al., 2020). It is also possible that there are other behavioural variables—other than problematic SNS use or unhealthy habits—that have a greater impact on their mental health, such as loneliness (Ausín et al., 2021).
To sum up, the Young Pessimist group scored the worst in terms of mental health (high depression and anxiety and low life satisfaction scores). This group was characterised by low optimism, the unhealthiest behaviours, and a high problematic SNS use, as well as a high percentage of people whose income had fallen. Based on these findings, it is reasonable to assume that this is the group with the most maladaptive coping strategies, where mental health is severely compromised. There was also a second group of young people, the Young Optimists who exhibited low mental health impairment (i.e. low levels of anxiety, depression and dissatisfaction with life). This group was characterised by high levels of optimism and low levels of maladaptive behaviours (i.e. problematic use of SNSs and unhealthy habits). There was a rather similar profile in the Optimistic Middle-aged group, with low levels of anxiety, depression and dissatisfaction with life, and low levels of maladaptive behaviours (i. e. problematic SNS use and unhealthy behaviours). This seems to suggest that behavioural variables and optimism are key variables for mental health protection in young and middle-aged adults. Another group that also exhibited poorer mental health was the Resilient Elders group, which was characterised by higher levels of resilience (but not optimism) and did not engage in unhealthy behaviours and problematic SNS use yet, it was not protected and showed high levels of anxiety, depression and low life satisfaction. For this group, it is not clear which variables put them at risk and which protect them, so further research is needed in this age group.
Finally, it is useful to describe the sociodemographic characteristics of the different groups. In terms of education, the Resilient Elders group were the group with the highest proportion of people who had university qualifications. In terms of living arrangement, the Resilient Elders had the highest proportion of people living alone or with a single cohabitant. When it comes to employment, it is worth noting that the Young Pessimists had the highest proportion of unemployed both before and during the lockdown. It was also the group with the highest percentage of income loss. Finally, caring for dependents was more common in the Middle-aged Optimists group, which is understandable given the average age of 45 and the fact that many of them will have dependent children or parents. The Young Pessimists group had the lowest proportion of relatives infected by or who died from COVID-19. However, the overall number of infected or dead relatives in the sample was very low (about 70% had no infected relatives and 92% have no relatives who died from COVID-19).
This study must be interpreted with certain limitations in mind. The first limitation is the use of a questionnaire (unhealthy habits) that was created ad hoc for the study due to the newness of the topic and had low reliability. It is also possible that other protective psychological variables such as mood were not assessed (Menéndez-Aller et al., 2020). Other variables related to the situation were not considered, such as COVID-19 fear (Ornell et al., 2020), COVID-19 anxiety (Arcieri, 2021), protective behaviours against infections (Padmanabhanunni & Pretorius, 2021), and the health habits of the population during the lockdown (Menéndez-Giménez et al., 2021). Moreover, as the data collection was conducted using an online questionnaire, this meant that it did not reach the part of the population who do not use the internet.
CONCLUSIONS
In short, it is possible to distinguish four coping groups according to the cluster analysis: 1) the Young Pessimists group, which scored the worst in terms of mental health (high depression and anxiety and low life satisfaction), and consisted of young people with low levels of optimism, high levels of unhealthy habits and problematic use of SNS; 2) the Young Optimists group, which scored the best in terms of mental health (low depression and anxiety and high life satisfaction), and consisted of young people with low levels of unhealthy habits and problematic use of SNS, as well as the highest level of optimism; 3) the Middle-aged Optimists group, which scored similarly to the previous group in mental health variables (low depression and anxiety and high life satisfaction). This group was characterised by an average age of around 45, and had low levels of problematic SNS use and unhealthy habits, as well as high levels of optimism, and 4) the Resilient Elders group, who had low mental health scores (high anxiety, depression and low life satisfaction). It consisted of older people, with below average levels of optimism, slightly above-average levels of resilience, low levels of problematic use of SNSs, and low levels of unhealthy habits. This study has implications for intervention and prevention as it highlights the different coping groups in an extreme scenario.
Author Notes:
Funding: This study did not receive funding.
Conflict of interest: The authors declare no competing interests.
REFERENCES
1. American Psychological Association (2014). The road to resilience. http://www.apa.org/helpcenter/road-resilience.aspx
2. Andreassen, C. S., & Pallesen, S. (2014). Social network site addiction—An overview. Current Pharmaceutical Design, 20(25), 4053-4061. https://doi.org/10.2174/13816128113199990616
3. Arcieri, A. A. (2021). The relationships between COVID-19 anxiety, ageism, and ableism. Psychological Reports, 125(5), 2531-2545. https://doi.org/10.1177/00332941211018404
4. Ausín , B., González-Sanguino, C., Castellanos, M. Ángel, Saiz, J., Ugidos, C., López-Gómez, A., & Muñoz, M. (2021). Soledad, salud mental y la COVID-19 en la población española. Escritos de Psicología, 14(2), 51-62. https://doi.org/10.24310/espsiescpsi.v14i2.12498
5. Balaban, D. C., & Spoaller, D. F. (2020). How social comparison on Instagram affects wellbeing. Perspectives from a study conducted during the lockdown. Studia Universitatis Babes-Bolyai, 65(2), 5-19. https://doi.org/10.24193/subbeph.2020.2.01
6. Baumgartner, J. N., Schneider, T. R., & Capiola, A. (2018). Investigating the relationship between optimism and stress responses: A biopsychosocial perspective. Personality and Individual Differences, 129, 114-118. https://doi.org/10.1016/j.paid.2018.03.021
7. Been, F., Emke, E., Matias, J., Baz-Lomba, J. A., Boogaerts, T., Castiglioni, S., Campos-Mañas, M., Celma, A., Covaci, A., Voogt, F., Her & Bijlsma, L. (2021). Changes in drug use in European cities during early COVID-19 lockdowns-A snapshot from wastewater analysis. Environment International, 153, Article 106540. https://doi.org/10.1016/j.envint.2021.106540
8. Boursier, V., Gioia, F., Musetti, A., & Schimmenti, A. (2020). Facing loneliness and anxiety during the COVID-19 isolation: The role of excessive social media use in a sample of Italian adults. Frontiers in Psychiatry, 11, Article 586222. https://doi.org/10.3389/fpsyt.2020.586222
9. Blanca, M. J., Alarcón, R., Arnau, J., Bono, R., & Bendayan, R. (2017). Non-normal data: Is ANOVA still a valid option? Psicothema, 29(4), 552-557. https://doi.org/10.7334/psicothema2016.383
10. Brailovskaia, J., Cosci, F., Mansueto, G., & Margraf, J. (2021). The relationship between social media use, stress symptoms and burden caused by coronavirus (Covid-19) in Germany and Italy: A cross-sectional and longitudinal investigation. Journal of Affective Disorders Reports, 3, Article 100067. https://doi.org/10.1016/j.jadr.2020.100067
11. Calina, D., Hartung, T., Mardare, I., Mitroi, M., Poulas, K., Tsatsakis, A., Rogoveanu, I. & Docea, A. O. (2021). COVID-19 pandemic and alcohol consumption: Impacts and interconnections. Toxicology Reports, 8, 529-535. https://doi.org/10.1016/j.toxrep.2021.03.005
12. Carriedo, A., Cecchini, J. A., Fernández-Río, J., & Méndez-Giménez, A. (2020). Resilience and physical activity in people under home isolation due to COVID-19: A preliminary evaluation. Mental Health and Physical Activity, 19, Article 100361. https://doi.org/10.1016/j.mhpa.2020.100361
13. Carver, C. S., Scheier, M. F., & Segerstrom, S. C. (2010). Optimism. Clinical Psychology Review, 30(7), 879–889. https://doi.org/10.1016/j.cpr.2010.01.006
14. Cong, D. D. (2021). The impact of fear and anxiety of Covid-19 on life satisfaction: Psychological distress and sleep disturbance as mediators. Personality and Individual Differences, 178, Article 110869. https://doi.org/10.1016/j.paid.2021.110869
15. Codagnone, C., Bogliacino, F., Gómez, C., Charris, R., Montealegre, F., Liva, G., Lupiáñez-Villanueva, F., Folkvord, F. & Veltri, G. A. (2020). Assessing concerns for the economic consequence of the COVID-19 response and mental health problems associated with economic vulnerability and negative economic shock in Italy, Spain, and the United Kingdom. Plos One, 15(10), Article e0240876. https://doi.org/10.1371/journal.pone.0240876
16. Cudo, A., Mącik, D., Griffiths, M. D., & Kuss, D. J. (2020). The relationship between problematic Facebook use and early maladaptive schemas. Journal of Clinical Medicine, 9(12), Article 3921. https://doi.org/10.3390/jcm9123921
17. Cuesta, M., Suárez-Álvarez, J., Lozano, L., García-Cueto, E. y Muñiz, J. (2018). Assessment of eight entrepreneurial personality dimensions: Validity evidence of the BEPE battery. Frontiers in Psychology, 9, Article 2352. https://doi.org/10.3389/fpsyg.2018.02352
18. Deontological Code of the Spanish Psychological Association (2010). Consejo General de Colegios Oficiales de Psicólogos. https://www.cop.es/index.php?page=CodigoDeontologico
19. Diener, E. D., Emmons, R. A., Larsen, R. J., y Griffin, S. (1985). The satisfaction with life scale. Journal of Personality Assessment, 49(1), 71-75. https://doi.org/10.1207/s15327752jpa4901_13
20. García-Fernández, L., Romero-Ferreiro, V., López-Roldán, P. D., Padilla, S., & Rodriguez-Jimenez, R. (2020). Mental health in elderly Spanish people in times of COVID-19 outbreak. The American Journal of Geriatric Psychiatry, 28(10), 1040-1045. https://doi.org/10.1016/j.jagp.2020.06.027
21. Gori, A., Topino, E., & Di Fabio, A. (2020). The protective role of life satisfaction, coping strategies and defense mechanisms on perceived stress due to COVID-19 emergency: A chained mediation model. Plos One, 15(11), Article e0242402. https://doi.org/10.1371/journal.pone.0242402
22. González-Nuevo, C., Cuesta, M., Postigo, A., Menéndez-Aller, A., García-Cueto, E. & Muñiz, J. (2023). Problematic social network use: Structure and assessment. International Journal of Mental Health and Addiction, 21, 2122–2137. https://doi.org/10.1007/s11469-021-00711-y
23. González-Nuevo, C., Cuesta, M., Postigo, Á., Menéndez-Aller, Á., García-Fernández, J., & Kuss, D. J. (2022). Using social networking sites during lockdown: Risks and benefits. Psicothema, 34(3), 365-374. https://doi.org/10.7334/psicothema2022.51
24. González-Sanguino, C., Ausín, B., Castellanos, M. Á., Saiz, J., López-Gómez, A., Ugidos, C., & Muñoz, M. (2020). Mental health consequences during the initial stage of the 2020 coronavirus pandemic (COVID-19) in Spain. Brain, Behavior, and Immunity, 87, 172-176. https://doi.org/10.1016/j.bbi.2020.05.040
25. Gundogan, S. (2021). The mediator role of the fear of COVID-19 in the relationship between psychological resilience and life satisfaction. Current Psychology, 40, 6291-6299. http://dx.doi.org/10.1007/s12144-021-01525-w
26. Gutiérrez-Hernández, M. E., Fanjul, L. F., Díaz-Megolla, A., Reyes-Hurtado, P., Herrera-Rodríguez, J. F., Enjuto-Castellanos, M. del P., & Peñate, W. (2021). COVID-19 lockdown and mental health in a sample population in Spain: The role of self-compassion. International Journal of Environmental Research and Public Health, 18(4), Article 2103. https://doi.org/10.3390/ijerph18042103
27. Haddad, J. M., Macenski, C., Mosier-Mills, A., Hibara, A., Kester, K., Schneider, M., Conrad, R. C., & Liu, C. H. (2021). The impact of social media on college mental health during the COVID-19 pandemic: A multinational review of the existing literature. Current Psychiatry Reports, 23(11), Article 70. https://doi.org/10.1007/s11920-021-01288-y
28. International Test Commission (2013). ITC Guidelines on Test Use. https://www.intestcom.org/files/guideline_test_use.pdf
29. Kira, I. A., Shuwiekh, H. A., Ashby, J. S., Elwakeel, S. A., Alhuwailah, A., Sous, M. S. F., Baali, S. B. A., Azdaou, C., Oliemat, E. M. & Jamil, H. J. (2021). The impact of COVID-19 traumatic stressors on mental health: Is COVID-19 a new trauma type. International Journal of Mental Health and Addiction. Advance Online Publication. https://doi.org/10.1007/s11469-021-00577-0
30. Keles, B., McCrae, N. & Grealish, A. (2020). A systematic review: The influence of social media on depression, anxiety and psychological distress in adolescents. International Journal of Adolescence and Youth, 25(1), 79-93. https://doi.org/10.1080/02673843.2019.1590851
31. Koliouli, F., & Canellopoulos, L. (2021). Dispositional optimism, stress, post-traumatic stress disorder and post-traumatic growth in greek general population facing the COVID-19 crisis. European Journal of Trauma & Dissociation, 5(2), Article 100209. https://doi.org/10.1016/j.ejtd.2021.100209
32. Lee, K., Jeong, G. C., & Yim, J. (2020). Consideration of the psychological and mental health of the elderly during COVID-19: A theoretical review. International Journal of Environmental Research and Public Health, 17(21), Article 8098. https://doi.org/10.3390/ijerph17218098
33. Lenhard, W., & Lenhard, A. (2016). Calculation of effect sizes. https://www.psychometrica.de/effect_size.html
34. Li, A., Wang, S., Cai, M., Sun, R., & Liu, X. (2021). Self-compassion and life-satisfaction among Chinese self-quarantined residents during COVID-19 pandemic: A moderated mediation model of positive coping and gender. Personality and Individual Differences, 170, Article 110457. https://doi.org/10.1016/j.paid.2020.110457
35. Liu, C. H., Zhang, E., Wong, G. T. F., & Hyun, S. (2020). Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: Clinical implications for US young adult mental health. Psychiatry Research, 290, Article 113172. https://doi.org/10.1016/j.psychres.2020.113172
36. Méndez-Giménez, A., Cecchini Estrada, J. A., Fernández Río, F. J., & Carriedo Cayón, A. (2021). Physical activity and prevention of depressive symptoms in the spanish population during confinement due to covid-19. Psicothema, 33(1), 11-117. https://doi.org/10.7334/psicothema2020.294
37. Nguyen, N. N. (2022). Optimism as a protective factor against alcohol use among Vietnamese teenagers. Journal of Substance Use, 27(4), 381-384. https://doi.org/10.1080/14659891.2021.1941358
38. Padmanabhanunni, A., & Pretorius, T. (2021). Behaviour is the key in a pandemic: The direct and indirect effects of COVID-19-related variables on psychological wellbeing. Psychological Reports, 125(5), 2456-2469. https://doi.org/10.1177/00332941211025269
39. Pérez-Rojo, G., López Martínez, J., Noriega García, C., Martínez Huertas, J. Á., Velasco Vega, C., Carretero Abellán, M. I., López-Frutos, P., Galarraga, L. & Pillemer, K. (2021). Older people’s personal strengths during the first wave of the COVID-19 pandemic. Psicothema, 33(3), 423-432. https://doi.org/10.7334/psicothema2020.453
40. Rogers, A. H., Shepherd, J. M., Garey, L., & Zvolensky, M. J. (2020). Psychological factors associated with substance use initiation during the COVID-19 pandemic. Psychiatry Research, 293, Article 113407. https://doi.org/10.1016/j.psychres.2020.113407
41. Rodríguez-Rey, R., Alonso-Tapia, J., y Hernansaiz-Garrido, H. (2016). Reliability and validity of the Brief Resilience Scale (BRS) Spanish version. Psychological Assessment, 28(5), e101-e110. https://doi.org/10.1037/pas0000191
42. Sandín, B., Valiente, R. M., García-Escalera, J., & Chorot, P. (2020). Impacto psicológico de la pandemia de COVID-19: Efectos negativos y positivos en población española asociados al periodo de confinamiento nacional. Revista de Psicopatología y Psicología Clínica, 25(1), 1–22. https://doi.org/10.5944/rppc.27569
43. Singleton, G., Johnson, L., Singleton, N., & Li, H. (2022). COVID-19-related anxiety: How do coping and optimism relate to substance use in African–American young adults? Journal of Community Psychology, 1– 18. https://doi.org/10.1002/jcop.22863
44. López-Núñez, M. I., Díaz-Morales, J. F., & Aparicio-García, M. E. (2021). Individual differences, personality, social, family and work variables on mental health during COVID-19 outbreak in Spain. Personality and Individual Differences, 172, Article 110562. https://doi.org/10.1016/j.paid.2020.110562
45. Menéndez-Aller, Á., Postigo, Á., Montes-Álvarez, P., González-Primo, F. J., & García-Cueto, E. (2020). Humor as a protective factor against anxiety and depression. International Journal of Clinical and Health Psychology, 20(1), 38-45. https://doi.org/10.1016/j.ijchp.2019.12.002
46. Ornell, F., Schuch, J. B., Sordi, A. O., & Kessler, F. H. P. (2020). “Pandemic fear” and COVID-19: Mental health burden and strategies. Brazilian Journal of Psychiatry, 42(3), 232-235. https://doi.org/10.1590/1516-4446-2020-0008
47. Osofsky, H. J., & Osofsky, J. D. (2013). Hurricane Katrina and the Gulf oil spill: Lessons learned. Psychiatric Clinics, 36(3), 371-383. https://doi.org/10.1016/j.psc.2013.05.009
48. Şahin, M. D. (2021). Effect of item order on certain psychometric properties: A demonstration on a Cyberloafing Scale. Frontiers in Psychology, 12, Article 590545. https://doi.org/10.3389/fpsyg.2021.590545
49. Salari, N., Hosseinian-Far, A., Jalali, R., Vaisi-Raygani, A., Rasoulpoor, S., Mohammadi, M., Rasoulpoor, S. & Khaledi-Paveh, B. (2020). Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Globalization and Health, 16(1), 1-11. https://doi.org/10.1186/s12992-020-00589-w
50. Sica, C., Latzman, R. D., Caudek, C., Cerea, S., Colpizzi, I., Caruso, M., Giulini, P. & Bottesi, G. (2021). Facing distress in Coronavirus era: The role of maladaptive personality traits and coping strategies. Personality and Individual Differences, 177, Article 110833. https://doi.org/10.1016/j.paid.2021.110833
51. Solé, B., Verdolini, N., Amoretti, S., Montejo, L., Rosa, A. R., Hogg, B., García-Rizo, C., Mezquida, G., Bernardo, M., Martínez-Aran, A., Vieta, E. & Torrent, C. (2021). Effects of the COVID-19 pandemic and lockdown in Spain: Comparison between community controls and patients with a psychiatric disorder. Preliminary results from the BRIS-MHC STUDY. Journal of Affective Disorders, 281, 13-23. https://doi.org/10.1016/j.jad.2020.11.099
52. Smith, B. W., Dalen, J., Wiggins, K., Tooley, E., Christopher, P., & Bernard, J. (2008). The brief resilience scale: Assessing the ability to bounce back. International Journal of Behavioral Medicine, 15(3), 194-200. https://doi.org/10.1080/10705500802222972
53. Stanton, R., To, Q. G., Khalesi, S., Williams, S. L., Alley, S. J., Thwaite, T. L., Fenning, A. S. & Vandelanotte, C. (2020). Depression, anxiety and stress during COVID-19: associations with changes in physical activity, sleep, tobacco and alcohol use in Australian adults. International Journal of Environmental Research and Public Health, 17(11), Article 4065. https://doi.org/10.3390/ijerph17114065
54. Terol, M. C., López-Roig, S., Rodríguez-Marín, J., Martí-Aragón, M., Pastor, M. A., & Reig, M. T. (2007). Propiedades psicométricas de la escala hospitalaria de ansiedad y depresión (HAD) en población española. Ansiedad y Estrés, 13(2-3). 163-176.
55. Urdiales-Claros, R., & Sánchez-Álvarez, N. (2021). Sintomatología depresiva e ideación suicida como consecuencia de la pandemia por la COVID-19. Escritos de Psicología, 14(2), 134-144. https://doi.org/10.24310/espsiescpsi.v14i2.12901
56. Vázquez, C., Duque, A., & Hervás, G. (2013). Satisfaction with life scale in a representative sample of Spanish adults: Validation and normative data. The Spanish Journal of Psychology, 16, Article e83. https://doi.org/10.1017/sjp.2013.82
57. Valiente, C., Contreras, A., Peinado, V., Trucharte, A., Martínez, A. P., & Vázquez, C. (2021). Psychological adjustment in Spain during the COVID-19 pandemic: Positive and negative mental health outcomes in the general population. The Spanish Journal of Psychology, 24, Article e8. https://doi.org/10.1017/SJP.2021.7
58. Vall-Roqué, H., Andrés, A., & Saldaña, C. (2020). The impact of COVID-19 lockdown on social network sites use, body image disturbances and self-esteem among adolescents and young women. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 110, Article 110293. https://doi.org/10.1016/j.pnpbp.2021.110293
59. Verdolini, N., Amoretti, S., Montejo, L., García-Rizo, C., Hogg, B., Mezquida, G., Rabelo-da-Ponte, F.C., Vallespir, C., Radua, J., Martínez-Aran, A., Pacchiarotti, I., Rosa, A. R., Bernardo, M., Vieta, E., Torrent, C. & Solé, B. (2021). Resilience and mental health during the COVID-19 pandemic. Journal of Affective Disorders, 283, 156-164. https://doi.org/10.1016/j.jad.2021.01.055
60. Vos, L. M., Habibović, M., Nyklíček, I., Smeets, T., & Mertens, G. (2021). Optimism, mindfulness, and resilience as potential protective factors for the mental health consequences of fear of the coronavirus. Psychiatry Research, 300, Article 113927. https://doi.org/10.1016/j.psychres.2021.113927
61. Weinberg, M. K., Seton, C., & Cameron, N. (2018). The measurement of subjective wellbeing: Item-order effects in the personal wellbeing index—adult. Journal of Happiness Studies, 19(1), 315-332. https://doi.org/10.1007/s10902-016-9822-1
62. Yesilyurt, F., & Turhan, N. S. (2020). Prediction of the time spent on Instagram by social media addiction and life satisfaction. Cypriot Journal of Educational Sciences, 15(2), 208-219. https://doi.org/10.18844/cjes.v15i2.4592
63. Zigmond, A. S. & Snaith, R. P. (1983). The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica, 67(6), 361-370. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x
RECEIVED: 9 de junio de 2022
MODIFIED: 2 de diciembre de 2022
ACCEPTED: 13 de diciembre de 2022